
By Cristan Williams
Installment Preface
Welcome to the ninth and last installment in this series on the rise and fall of Disco Sexology. In the previous installment, I interviewed the author of the classic, The Last Time I Wore a Dress, Dylan Scholinski. Scholinski was diagnosed with Gender Identity Disorder and confined to a mental institution that sought to convert him into a cisgender girl through makeup lessons and other gender-related “therapies.”
On the Ethics of Sacrificing Children on the Altar of an Ideology
“…freedom to create and to construct, to wonder and to venture. Such freedom requires that the individual be active and responsible, not a slave or a well-fed cog in the machine…It is not enough that men are not slaves; if social conditions further the existence of automatons, the results will not be love of life but love of death.”
For me, the shocking truth revealed by Disco Sexology history is the corrosive hubris of an uncritical ontology that functioned for decades as axiomatic circular reasoning. Over and over again, I’ve heard trans people who were subject to Disco Sexology describe their experience as “soul-killing” or “destructive.” At its core, Disco Sexology structurally aligns itself with the very cultural forces that inspires despair for the patient. The ontological architecture of Disco Sexology overtly validates that the cultural gender identity binary is the optimal way of experiencing one’s humanity.
From the moment a patient steps into the office of a Disco Sexologist, the patient’s experience is contextualized as problematic, pathological, and ultimately incompatible with optimal well-being. Such a positioning of the patient’s experience of self is an act of objectification, not actualization. Indeed, Disco Sexology seems primarily centered upon the problems others have or may have with the patient’s gender expression or identity, turning other’s gender discomfort into a clinical feature of the patient’s embodied selfhood.
The ontological power structure of Disco Sexology ensures a hierarchical patient-therapist interaction:
- The Disco Sexologist examines; the patient is examined.
- The Disco Sexologist knows the optimal nature of the patient’s being; the patient does not.
- The Disco Sexologist conducts “therapy” by producing optimal insights concerning the nature of the patient’s being; the patient receives these insights.
- The Disco Sexologist directs context and experience; the patient complies.
- The Disco Sexologist directs the scope of therapeutic content; the patient adapts to it.
- The Disco Sexologist is the functional subject of the therapeutic relationship while the patient is the functional object.
Such power relationships attempt to modulate the patient’s selfhood for the benefit of those who are uncomfortable with non-normative experiences of gender. Moreover, it serves to estrange the patient from their experience of self, normalizing the objectification of self. Thus, the “therapy” the patient receives from the Disco Sexologist primarily concerns itself with optimizing the patient’s gendered value within culture.
The ideas Dr. Zucker’s CAMH promoted dialectically orbited an ontology of gender order and disorder that was constructed through an, in the words of the CAMH Director, “very strong charismatic leader who everybody follows.” As this self-referential ontology was deployed and asserted through academic and psychiatric sources controlled by opinion leaders of Disco Sexology, it asserted a circular logic that privileged traditional modes of gender identity as clinically optimal through hierarchical power relationships between patient and clinician that was constitutionally incapable of recognizing or responding to iatrogenic trauma. Indeed, in some sense, the entire phenomena of “gender identity disorder” is iatrogenic in nature.
Disco sexology constructs therapy around questioning the patient’s subjective experience of their gender identity rather than the patient’s experience of cultural gendered norms. While we know that the majority of mental health problems –from depression to suicidal ideation– is a result of the traumas society heaps upon the patient, Disco Sexology, in a sense, colludes with that society in problematizing the patient’s experience of gender identity. In this way, a defining feature of Disco Sexology is its investment in training the patient to accept the gendered modes of being culturally assigned to them at birth.
To highlight the passion with which Disco Sexology advocates have protected their ontological power-knowledge, consider the experience of Dr. Milton Diamond, a sexologist who dared question the gender research of Disco Sexologist Dr. John Money, as recounted in the book, As Nature Made Him: The Boy Who Was Raised as a Girl:
“I was sitting with some people over at one end of the room,” Diamond recalls, “and Money was sitting over in another part of the room with Anke Ehrhardt. And all of a sudden he gets up and shouts at the top of his voice, ‘Mickey Diamond, I hate your fucking guts!’”
An altercation ensued.
“They were arguing over the twins case,” says Vern Bullough, then a professor at the State University of New York at Buffalo, and a friend of both men. “Mickey pointed out to John that all the data was not there, that it was too early to draw definitive conclusions about the kid. John suddenly slugged Mickey. Hit him. Mickey did not fight back. He just repeated, ‘The data is not there.’ John yelled at him, ‘We have to stick together as sex researchers and not challenge one another!’”
I interviewed Dr. Diamond about this incident:
Cristan Williams: I understand that there’s a myth concerning you and Dr. Money. The myth is that during a conference, Money got very angry with you and physically tried to attack you. Is there any truth to that story?
Milton Diamond: Oh, there is definite truth to that! The only problem is, I don’t remember –some people remember [Dr. Money] as having struck the blow– I don’t remember his having struck the blow. So, there’s that, but otherwise, that’s a very vivid memory.
Williams: Some have said that this represents one of the epic rivalries in research. For you, what was the thing about Money’s research that bothered you?
Diamond: First of all, you have to understand that he was the big guru and I was a graduate student at the time. So, I wrote a critique of his paper and of his ideas… I thought that Money’s ideas were wrong and I described and discussed it intellectually. I submitted it to the Quarterly Review of Biology… now, to me, I love research and I look at research with a capital ‘R’, but Money took it as a big insult because it attacked him. So, he was the one who got angry with me; I couldn’t care less. I didn’t even know the gentleman at the time… I was arguing against his thesis; I wasn’t arguing against him as a person, but he took it personal. I’d never met him until that meeting where he stood up and expressed his anger… You have to understand, he would never contact me directly, but he wrote many things that were defamatory not only against me, but against anyone who criticized him and his work, were fair game for his diatribes.
This altercation centered around the opinions Dr. Money promoted to justify his asserted gender ontology, regardless of the difficulties Money’s power-knowledge created for David Reimer and his family.
Watch the documentary titled, Dr. Money and the Boy with no Penis here.
Disco Sexology’s theoretical foundation –that is, the experience of transition is predicated upon actualizing a fantasy of cultural gender conformity– is an unproven postulation that structurally defined all subsequent interactions with the trans population. From its advancement in the 1970s, this ontological view of the trans experience informed every aspect of trans research and care, ultimately functioning as a form of governmentality through the state-run CAMH gender program. CAMH sexologist opinion leaders went on to inform the way the DSM-IV regarded the trans experience which, in turn, defined the way psychological professionals engaged the trans community around the globe.
The entire purpose of physical transition, according to Disco Sexology advocates, is to merely facilitate a movement from one cultural gender role to its culturally asserted opposite. Such myopic caricatures of the trans experience are incapable of accounting for butch trans women or effeminate trans men. If such is the case for the trans community, what are we to make of the decades of trans activism focused on breaking down the gender binary?
As someone who regularly presents for university students, I try to ensure that my audience knows that when “gender identity” is used in trans discourse, it may be referencing any one of three categories:
A.) One’s subjective experience of one’s own sexed attributes;
B.) One’s sexed identification within the context of a social grouping; or,
C.) Both A and B
When I discuss these categories, I’m describing the nuances between the experience of self as it relates to the body (A), the experience of self as it relates to social groupings (B), and their intertextual relationship (C). In other words, I am noting the subtle differences between the subjective experience of having a body, the binary categories we culturally force bodies into, and the tension between these two experiences.
Disco Sexology seems to be incapable of distinguishing between the nuances of identity and role. Should I speak in terms of identity, I am speaking in terms of form; should I speak in terms of role, I am speaking in terms of function. For Categories A, B and C, I am speaking of form or, in other words, that which relates to the subjective experience of being, not doing. Trans author Jan Morris wrote of the insidious interplay of identity and role in her 1974 book Conundrum:
The more I was treated as a woman, the more woman I became. I adapted willy-nilly. If I was assumed to be incompetent at reversing cars, or opening bottles, oddly incompetent I found myself becoming. If a case was thought too heavy for me, inexplicably I found it so myself. Thus as I now found myself far more into the company of women than of men, I began to find women’s conversation in general more congenial. Women treated me with a frankness which, while it was one of the happiest discoveries of my metamorphosis, did imply membership of a camp, a faction, or at least a school of thought; and so I found myself gravitating always towards the female, whether in sharing a railway compartment or supporting a political cause. Men treated me more and more as a junior, as the Chevalier D’Eon had been obliged to accept a guardian in his womanhood — my lawyer, in an unguarded moment one morning, even called me “my child;” and so, addressed every day of my life as an inferior, involuntarily, month by month I accepted this condition. I discovered that even now men prefer women to be less informed, less able, less talkative, and certainly less self-centered than they are themselves; so I generally obliged them.1
It’s clear that even in the 1970s, trans people were giving voice to the nuances of identity and role. Morris described her 1960-era experience of being placed into the sex class woman as “involuntary” even though she had a confounding awareness of what was happening to her. As men acted out their maleness upon Morris, she found herself to be “inexplicably” attenuated within her culture. The gender conditioning Morris faced was predicated upon a culture invested in constructing, enforcing, and perpetuating a social gender binary. Disco Sexology presumes that the experience Morris described is, in fact, the goal of transition.
Here, Morris describes an experience of gender that’s intelligible to practically everyone: gender role conditioning and our contextualization of that experience. While some might cast Disco Sexologists as being intentionally cruel, it seems the cisgender therapists who created Disco Sexology focused on the aspect of gender that they themselves were intimately familiar with: gender role. Given the power relationship between the therapist and patient Disco Sexology perpetuates, I find it unsurprising that the eminent men and women of Disco Sexology believed their experience of gender role must be the basis for the trans and intersex experience.
I think there’s a very good reason that when Zucker –confronted by his peers during his 2016 presentation against laws banning conversion therapy– remarked that he didn’t understand the critiques he was facing, the audience responded in exasperation, “That’s the problem!” From a Disco Sexology perspective, contemporary best practices are, in a functional sense, incomprehensible. Gender therapy situated around the affirmation of gender expression –in whatever form that takes– is an approach that’s contrary to the ontological worldview of Disco Sexology activists. Affirming therapeutic models offer a patient-therapist relationship wherein the patient’s gender isn’t problematized and pathologized.
Even so, trading on the very power relationships cultivated over decades, Disco Sexology advocates regularly take to the media, warning a largely cisgender population of the asserted dangers of “transgender advocates” who will inevitably wreck the lives of youth the Sexologists claim they could have otherwise saved.
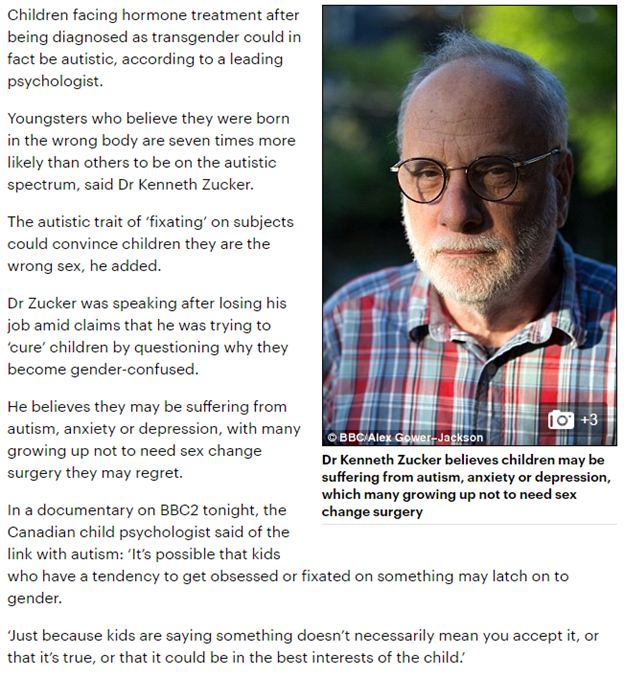
In January 2017, the BBC recently featured a documentary entitled, Transgender Kids: Who Knows Best? The documentary featured the work of Dr. Zucker who asserted that trans kids may be autistic and could benefit from treatment protocols focused on autism. Prior to the airing of the documentary, more than 10,000 people urged the producers of the documentary to allow affirmative therapists to preview the film to ensure the BBC wouldn’t unwittingly spread the very fear and misinformation that’s been the critical focus of this article.2In an apparent denial of a requested review, the executive producer of the documentary, Sam Bagnall assured the creators of the petition that, “great care has been taken to ensure that this programme meets our editorial guidelines,” and that the documentary was “fair, balanced and presents a range of views.” The BBC’s own description of the documentary stated that the documentary focuses on Dr. Zucker and that it, “challeng[es] the new orthodoxy that children know best.” The description continues:
Speaking on TV for the first time since his clinic was closed, Dr. Kenneth Zucker believes he is a victim of the politicisation of transgender issues. The film presents evidence that most children with gender dysphoria eventually overcome the feelings without transitioning…
The attentive reader will recall that, in fact, the CAMH gender program was not closed upon Dr. Zucker’s departure and might wonder why this false narrative is important to the BBC documentary message.
While the documentary producer declined to allow the film to be reviewed by experts in contemporary best practices, media representatives were given advanced quotes from the documentary, producing the following examples of media coverage:
What power stance must one have to encourage parents who watch the BBC presume their trans kids are like children engaging in anthropomorphic schoolyard play? What level of hubris must one attain to view such assertions as helpful to trans children?
A mother of three cis children and one trans child who appeared on the documentary accused the show of lying to her in order to trick her into being interviewed for the program. She said, “I’m absolutely disgusted. The producers definitely deceived us… The synopsis is obviously one-sided. I can see they baited me.” She went on to say:
That synopsis is embarrassing and hurtful to us as a family. It’s shaming us and saying we did the wrong thing… This synopsis for the documentary is like throwing everything back in [my trans daughter’s] face. Did they think we were a joke? Were they laughing at us while we thought we were doing a good thing? It’s very insulting.
Prior to the documentary airing, the BBC featured Dr. Ray Blanchard promulgating the very confusion of identity and role featured in Green’s The Sissy Boy study. On BBC’s Newsnight, Blanchard asserted:
Every follow up study has shown that the majority of children with gender identity issues do not end up transsexual. The majority end up with normal gender identity. The first line of approach clinically should be helping the child accept his or her sex. If they can’t do that, then by puberty it’s reasonable to consider puberty blockers.
The objective data show the rates of suicidal ideation and gestures in gender dysphoric children are the same as the rates of those gestures and ideation in other psychiatric populations of children and adolescents. Some parents are being emotionally blackmailed by false information about threats of suicide by gender dysphoric children into thinking that if they make any attempt to help their kid accept their anatomical sex, that they are putting their child at risk of suicide. It’s pure manipulation by trans activists.
Here, Blanchard promoted the selfsame confused clinical metrics he helped pioneer in the DSM-IV: lumping a very large sample of gender-expansive kids in with a small sample of gender dysphoric children, leading to the contrived finding that “most” children do not wind up transsexual. He does not note –indeed, he cannot, as a matter of ontology, note– that most of the children in the group of which he speaks never had gender dysphoria, to begin with. Moreover, he fails to mention that his previous CAMH colleague, Dr. Zucker himself asserted that 70% of the children he treated for Gender Identity Disorder at the clinic did not have gender dysphoria.
Moreover, why would Blanchard not mention published research which contradicts his “false information” claim? Would not the following conclusion from a 2016 pediatric study be pertinent to the information Blanchard was presenting to the public?
Socially transitioned transgender children who are supported in their gender identity have developmentally normative levels of depression and only minimal elevations in anxiety, suggesting that psychopathology is not inevitable within this group. Especially striking is the comparison with reports of children with GID; socially transitioned transgender children have notably lower rates of internalizing psychopathology than previously reported among children with GID living as their natal sex.
When the vast majority of the patient population Blanchard was speaking of does not have gender dysphoria, why did he take to a government media outlet to assert that the very first thing gender clinics should focus on is getting patients to “accept his or her sex?” What does it mean to invest clinical effort in convincing non-gender dysphoric patients –that is, the 70% of patients who did not have issues with their sexed attributes at Dr. Zucker’s clinic– to accept their sexed attributes? What might we infer about the clinical experience of the other 30% of the patient population with gender dysphoria? When 70% of the patients Dr. Zucker treated for gender identity disorder didn’t have gender dysphoria in the first place, what are we to make of Disco Sexology claims that the majority of patients treated for gender identity disorder did not go on to transition? Consider the public assertions of Blanchard to the assertions Zucker himself made about his patient population, data that was, by the way, not featured in the documentary:
[A]t age 3, children begin to self-label and form their gender identity. Nascent signs often emerge before age 18 months and perception of gender is present and forming […] [a]t age 15 in adolescence the most likely outcome is persistence of the GD. 70%-80% would continue to have GD. The treatment would be social transition and biomedical treatment.
However, the documentary opens with a voiceover asserting:
Around the world, the transgender community is on the march. Parents are facing an explosion in the number of children saying they were born in the wrong body. We are now told to believe children and support them changing gender. One top expert has now been fired for challenging the idea that children know best. Parents face terrifying choices and the stakes could not be higher.
Within the first minute and a half, the documentary featured Blanchard asserting, “The adult transsexual community tried to intervene in the destinies of children who aren’t even their own.” while Zucker asserted, ‘A four-year-old might say that’s he’s a dog. Do you go out and buy dog food?” The documentary then spent the next 10 minutes constructing the following narrative:
For three decades, Zucker and his team treated more than a thousand children at Toronto’s child gender clinic at the Centre for Addiction and Mental Health, CAMH. He doesn’t agree with the gender-affirmative approach promoted by many transgender activists. “Identity is a process. It’s complicated. It takes a long period of time, in a sense, to know who a child really is. A four-year-old might say that he’s a dog. Um…do you go out and buy dog food?” [..] Zucker became a target for transgender activists, who have increasingly influenced policy in Canada. [Zucker said,] “I completely reject the allegation that I’ve ever practiced conversion therapy. I practice what I would call developmentally-informed therapy.”
In June 2015, supported by gender-affirmative doctors, Cheri DiNovo pushed through a new law banning conversion therapy in Ontario. A review was launched into Zucker’s clinic and six months later, it was shut down. Banning conversion therapy has had a huge impact. In fact, the impact is still being felt. One of our largest mental health institutions changed their entire programming, scrapped what they were doing, started again. Dr. Kenneth Zucker, one of the world’s leading authorities on gender dysphoria, was fired.
The documentary closes, stating the following concern:
Expressing doubt about the gender-affirmative approach to children is now risky. Accusations of transphobia are common. In Canada, one of the world’s leading authorities on gender dysphoria was fired. A lot of people who are professionals, and would be perfectly willing in private to say that they’re appalled by Ken Zucker’s firing, would be terrified to say that in public for fear of their own jobs, or being treated as pariahs by their co-workers.
Without the benefit of the decades of context featured in this article, what conclusions might a BBC audience have about affirmative therapy? Laypeople, writing for major media outlets geared towards the general public, regarded the information presented in the documentary to be balanced and informative:
However, those with a more complete understanding of Disco Sexology’s history were not so credulous. After watching the documentary, Dr. Dan Karasic, Clinical Professor of Psychiatry at the University of California wrote in a Facebook post:
The documentary was peculiar, in that it purported to be about the topic of trans kids, but in fact, it was about CAMH. Several of Dr. Zucker’s supporters at CAMH and a few of his critics in Toronto were interviewed, though there were no specifics about the firing. If the documentary were meant to be about the larger topic of trans kids, why weren’t child psychologists and child psychiatrists outside of CAMH interviewed? Why weren’t child psychologists and child psychiatrists doing research with trans kids in the US or the Netherlands interviewed? The show featured someone with regret, but that person had a father (who was interviewed) who did not support early social transition, and that person had chest surgery as an adult, at 20 years old, so it was unclear how that related to the issue of parents allowing their children to socially and medically transition. And why weren’t any people harmed as children by conversion therapy or by non-supportive parents interviewed? Or Kristina Olson, Ph.D., and her study subjects, who are being followed longitudinally?
After the BBC documentary aired, supporters of Disco Sexology assailed Dr. Stuart Lorimer, psychiatrist, and expert on gender dysphoria, alleging that he was part of the transgender agenda, therefore ruining the lives of children. In exasperation, he pinned the following tweet to his Twitter:
Echoing the frustration of Karasic, the Chairperson of Coventry Pride, Paul Desson-Baxter wrote on his Huffington Post blog:
In my opinion there was no balance to it and it was biased towards the denial of trans+ children. It also seemed to scare mongered to a stupid degree the idea that once a child said they were trans a vampiric group of clinicians, therapists and trans activists would descend and never let the child change their mind, and force them to take puberty blockers, then hormones and make them have surgery, all of which couldn’t be further from the truth. Young trans people I know have had to fight tooth and nail to prove their transness to get anything.
While trans people have responded to the narrative pushed by the BBC documentary, it seems that those swayed by the documentary support of Disco Sexology view such responses as proof that the transgender agenda is oppressing Disco Sexologists and their activists. If anything, Disco Sexologists like Blanchard seems energized by his reception in the media:

In light of the general public’s positive reception of the BBC’s documentary, a new petition was launched asking that the documentary be shown to an American audience. The petition reads: “We want the BBC to air and stream “Transgender Kids: Who Knows Best?” for American viewers!”
“Transgender Kids: Who Knows Best?” investigates the practices of the now closed CAMH Child Youth and Family Gender Identity Clinic under the leadership of Dr. Kenneth Zucker. This documentary allows Dr. Zucker, his staff, and families who received treatment at the clinic to explain the paradigm the clinic practiced of developmentally informed care for childhood gender dysphoria. The approach of the staff of Dr. Zucker has been maligned by trans activists as “reparative therapy” which sought to prevent a child from choosing medical interventions to affirm a trans identity. Trans activists ultimately targeted Dr. Zucker with false claims about inappropriate comments to a patient and continue to spread libelous, demonstrably false stories about the care he and his staff provided.
Dr. Zucker, his staff, and families who received care at the clinic dispute the claim that care that respects the cognitive and emotional development of children is “reparative therapy” which seeks to prevent medical transition. They speak to a clinically informed view that the possibilities for discernment of a permanent trans identity and deep self knowledge are different for children of different levels of development. It is important that Americans, especially families seeking to understand how to support children with gender dysphoria, are given detailed information about Dr. Zucker’s approach beyond the incorrect claims of trans activists. More information, rather than less, is needed by individuals making decisions about how to approach their gender dysphoria, and family members seeking to support their children experiencing gender dysphoria. For the well being of individuals who experience gender dysphoria, and for the loves ones who wish to support them, it’s important this program is aired in America.

The history of Disco Sexology is littered with the destruction wrought from an obtuse hubris that’s incapable of recognizing the iatrogenic effects of its circular logic. Dr. Money would rage at and slander those who dared question his ontology and in doing so, sacrificed the life David Reimer might have had. What of the forgotten life and death of Kirk Murphy, a recipient of Drs. Green and Rekers’ behavioral gender treatment? What more is Disco Sexology willing to sacrifice in its ongoing fight to promote and protect its power-knowledge? ⬛
Acknowledgments
I wish to thank all of those who helped me with this article. Many heartfelt thanks to those who were open to interviews for this article: Dr. Kwame McKenzie, Dr. Colton Keo-Meier, Arlene Lev, Dylan Scholinski, and especially Erika Muse. Thank you for the research assistance from Drs. Kelley Winters, Stan Monstrey, Peggy Cohen-Kettenis, Allen Frances, and Hannah Decker. Thank you to all those who helped review this article: Marti Abernathey, Kelly Winters, Monica Roberts, Dr. Lauren Chamoix, Denise Norris, Kat Rose, Alexis Melvin, and Margo Schulter.
Kwame McKenzie, MD: Dr. McKenzie is Director of Health Equity at CAMH. He is a full Professor and the Co-Director of the Division of Equity Gender and Population in the Department of Psychiatry at the University of Toronto. Dr. McKenzie is also CEO of the Wellesley Institute and a member of the Mental Health and Addictions Advisory Council to the Minister of Health. He sits on the Board of the United Way Toronto and the Ontario Hospitals Association.
Arlene Lev, LCSW-R, CASAC: Lev is the Clinical Director of Choices Counseling and Consulting and the Director of TIGRIS – the Institute for Gender, Relationships, Identity, and Sexuality in Albany NY, and on the faculties of numerous colleges and universities. She is currently completing a book with Andrew Gottlieb called Families in Transition: Parent Perspectives on working with gender nonconforming children and transgender youth.
Colton Keo-Meier, Ph.D.: Dr. Keo-Meier is a Houston-based psychologist who specializes in working with sexual and gender minorities, their families, and individuals questioning their sexual identity and/or gender identity. He is a co-founder of Gender Infinity, an organization dedicated to connecting gender diverse individuals and their families with affirmative resources in the southern United States.
Dylan Scholinski: Scholinski is a distinguished artist, author, and public speaker and has appeared on 20/20, Dateline, and Today to discuss his experiences and has been featured in a variety of newspapers and magazines. Recently his award-winning book, The Last Time I Wore a Dress: A Memoir was listed in the Top 10 Must Reads in Out Magazine’s first transgender issue. His work not only portrays the anguish of his hospital years but also his ultimate triumph.
I wish to give a very special thanks to the courageous Erika Muse for sharing her experience with Dr. Zucker’s treatment: From the bottom of my heart, thank you for sharing your experience with me and with the world.

- Morris, Jan. 2002. In Conundrum, 149. New York: New York Review of Books.
- At the time of writing this article, 10,593 people had signed a petition titled, ‘Transgender Kids: Who Knows Best?’ should not be broadcast until reviewed by experts.



great series thank you.