While there are many who feel that morality must be built into law, I believe that the elimination of transsexualism is not best achieved by legislation prohibiting transsexual treatment and surgery but rather by legislation that limits it and by other legislation that lessens the support given to sex-role stereotyping, which generated the problem to begin with. Any legislation should be aimed at the social conditions that initiate and promote the surgery as well as the growth of the medical-institutional complex that translates these stereotypes into flesh and blood. More generally, the education of children is one case in point here. Images of sex roles continue to be reinforced, at public expense, in school textbooks. Children learn to role play at an early age.
– Raymond (1980), Technology on the Social and Ethical Aspects of Transsexual Surgery
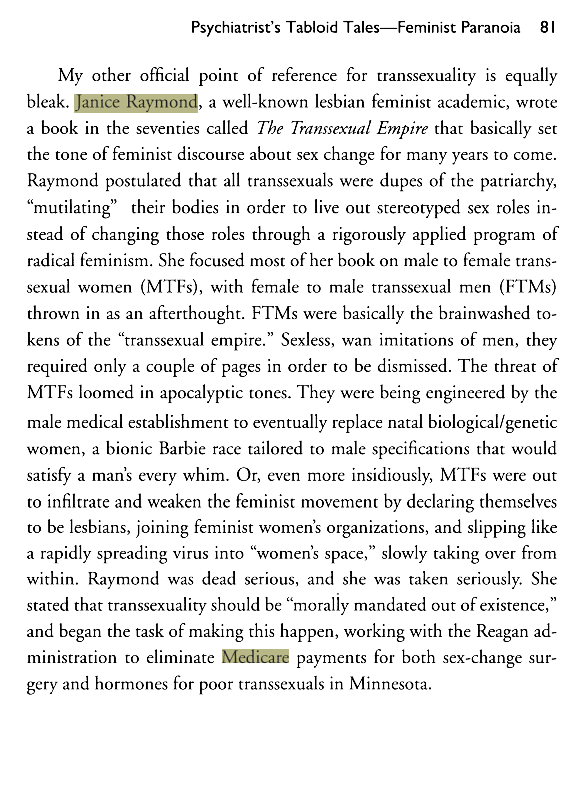
The TERF movement played a significant role in the revocation of trans healthcare access. In fact, TERF activist, Janice Raymond, authored the government’s anti-trans position.
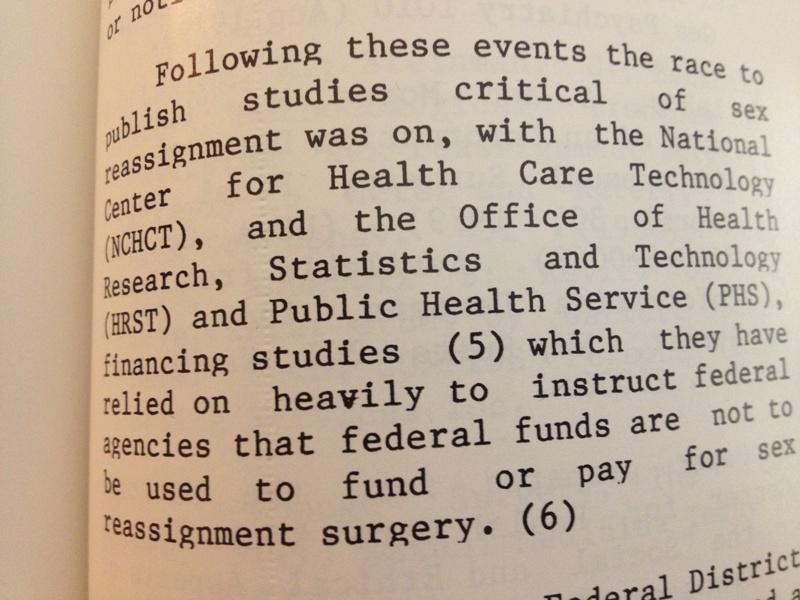
The National Center for Healthcare Technology was a government funded body that reviewed metadata so that Health & Human Services (HHS) would be able to make evidence-based judgements about the efficacy of medical technologies. In short, they informed the US government on what was and what was not medically efficacious. The NCHCT had Janice Raymond, author of The Transsexual Empire: The Making of the She-Male issue their position on the efficacy of trans medical care in a paper titled, “Technology on the Social and Ethical Aspects of Transsexual Surgery.” This position paper makes practically all the same assertions about trans people commonly found in far right-wing anti-trans propaganda; however, unlike other extremist group propaganda, this misleading report informed HHS’ position on trans medical care. The report was available through the Office of the Associate Director for Medical and Scientific Evaluation, Public Health Service.
Raymond asserted that trans medical care was a new phenomena, unethical, asserted that legislation should block trans medical care and that it would be best to institute a national program of reparative therapy.
Until Raymond’s HHS paper, the US government supported trans care as medically necessary. I want you to reread that previous sentence. This meant that poor trans people could freely access psychological and medical care and it meant that public and private insurers had no basis upon which to reject coverage of trans care.
It was only after the NCHCT pushed Raymond’s bigotry in 1980 that the US government reversed course in 1981 and took up Raymond’s views and rhetoric. Raymond’s hate became the government’s stance. Raymond – a Catholic ethicist, not a clinician – was the architect of the anti-trans stance the US government adopted in the 1980s. This official anti-trans stance soon spread to private insurers and the American trans population soon found itself without access to medically necessary health care.
There’s a reason many trans people lay the death and suffering of untold numbers of trans people at the feet of Janice Raymond, PhD.
In a time when employment discrimination against trans people became legal, Raymond helped dismantle the trans community’s ability to access trans health care through public and private insurance. Raymond heralded in the era in which trans people (many to most of whom were unemployed, depending upon the study) had to pay out of pocket or go without. In essence, Raymond helped ensure the future of a medical system that was unresponsive to the needs of the trans community at every level.
How many trans people have taken their lives because they were not able to access the medically necessary psychological and medical they needed? How many trans people died as a result of their encounter with an unresponsive and transphobic medical system?
One of the most severe results of denying coverage of treatments to transgender insureds that are available to non-transgender insureds is suicidal ideation and attempts.
A meta-analysis published in 2010 by Murad, et al., of patients who received currently excluded treatments demonstrated that there was a significant decrease in suicidality post-treatment. The average reduction was from 30 percent pretreatment to 8 percent post treatment.
De Cuypere, et al., reported that the rate of suicide attempts dropped dramatically from 29.3 percent to 5.1 percent after receiving medical and surgical treatment among Dutch patients treated from 1986-2001.
According to Dr. Ryan Gorton, “In a cross-sectional study of 141 transgender patients, Kuiper and Cohen-Kittenis found that after medical intervention and treatments, suicide fell from 19 percent to zero percent in transgender men and from 24 percent to 6 percent in transgender women.)”
Clements-Nolle, et al., studied the predictors of suicide among over 500 transgender men and women in a sample from San Francisco and found a prevalence of suicide attempts of 32 percent. In this study, the strongest predictor associated with the risk of suicide was gender based discrimination which included “problems getting health or medical services due to their gender identity or presentation.”According to Gorton, “Notably, this gender-based discrimination was a more reliable predictor of suicide than depression, history of alcohol/drug abuse treatment, physical victimization, or sexual assault.”
A recent systematic review of largely American samples gives a suicide attempt rate of approximately one in every three individuals with higher rates found among adolescents and young adults. According to Dr. R. Nicholas Gorton, MD, who treats transgender people at a San Francisco Health Clinic, “The same review also noted that while mental health problems predispose to suicidality, a significant proportion of the drivers of suicide in the LGBT population as a whole is minority stress.” He continues to conclude that, “[f]or transgender people such stress is tremendous especially if they are unable to ‘pass’ in society. Surgical and hormonal treatments — that are [also] covered for non-transgender insureds — are specifically aimed at correcting the body so that it more closely resembles that of the target gender, so providing care significantly improves patients’ ability to pass and thus lessens minority stress.”
These studies provide overwhelming evidence that removing discriminatory barriers to treatment results in significantly lower suicide rates.
– State of California Department of Insurance, 2012
The ghost Janice Raymond’s hard work is still alive today. TERFs continue to advocate against any movement away from the medical landscape Raymond wrought. Even in 2013, 33 years after Raymond’s successful effort to dismantle trans healthcare, trans people continue to suffer each and every day.
Even though the American Medical Association, American Psychological Association, American Academy of Family Physicians, National Association of Social Workers, World Professional Association for Transgender Health, National Commission on Correctional Health Care, American Public Health Association, American College of Obstetricians and Gynecologists all agree that trans care is medically necessary, trans people still endure under the TERF movement’s yoke.



Small correction – the title is “Paper Prepared for the National Center for Health Care Technology
on the Social and Ethical Aspects of Transsexual Surgery”
What is most scandalous is that this situation continues today. Only now is it being reviewed and its evidential basis re-examined.
The whole argument is based on ideology, not medicine. For example (from the report)
Beginning in order with the list of sex distinctions, the most important reality is that it is biologically impossible to change chromosomal sex. If chromosomal sex is taken as the bottom line of maleness or femaleness, the male who undergoes sex conversion surgery is NOT female.
Except now we know “chromosomal sex” gets changed via bone marrow transplant: see
Bone marrow-derived cells from male donors can compose endometrial glands in female transplant recipients by Ikoma et al in Am J Obstet Gynecol. 2009 Dec;201(6):608.e1-8
We also know that “chromosomal sex” is not reliable, even in the most conservative and reactionary ideological sense. 1 in 300 men aren’t 46,XY, some women are. Rarely so are the daughters they give birth to.
J Clin Endocrinol Metab. 2008 Jan;93(1):182-9
A 46,XY mother who developed as a normal woman underwent spontaneous puberty, reached menarche, menstruated regularly, experienced two unassisted pregnancies, and gave birth to a 46,XY daughter with complete gonadal dysgenesis.
That the objection is purely ideological, even religious, is shown by this telling admission about medical effectiveness in the report:
For this small number of individuals, transsexual surgery is not only a therapeutic necessity but a reasonable and humane treatment. Furthermore, the majority of postoperative reports of transsexuals testify that the surgery has been proven effective and efficacious and is therefore no longer experimental. They cite the fact that 90% of those persons who have undergone surgery report that their lives are happier and healthier.
The report then says that despite the treatment not being “experimental” in an objective sense, it should be considered “experimental” anyway, because ideology.
Again, that this situation has been allowed to continue for so long, superstition and provably false pseudo-scientific woo used as a basis for over-ruling scientific evidence and fact-based medicine is scandalous. Outrageous. It should have been caught and corrected decades ago.