
Dr. Littman lies, possibly misleading parents into withholding care from trans kids.
Recently the author of a Rapid Onset Gender Dysphoria (ROGD) study lied to a credulous Canadian reporter who printed misleading medical and psychological information that can encourage parents to withhold evidence-based care from their children. The following is an excerpt from Canada’s The Globe and Mail newspaper:

Dr. Littman describes the condition experienced by these girls as “rapid-onset gender dysphoria” (ROGD). It develops during or soon after puberty and mainly affects girls with no previous signs of childhood gender dysphoria. Many, however, do have a history of mental illness, and some are on the autism spectrum. The most controversial element of Dr. Littman’s research is her claim that ROGD spreads via social and peer contagion.
ROGD also spreads by social media according to Dr. Littman; some parents describe their daughters binge-watching YouTube transition videos. “It is plausible that online content may encourage vulnerable individuals to believe that nonspecific symptoms and vague feelings should be interpreted as gender dysphoria stemming from a transgender condition,” Dr. Littman writes in her research article.
Ray Blanchard thinks ROGD is real. Dr. Blanchard is a professor of psychiatry at the University of Toronto who spent many years working in a gender identity clinic. He says Dr. Littman’s problem is that she has challenged some sacred taboos. “The idea that social influences may be involved flies in the face of the ‘born that way’ or ‘you are who you say you are’ narrative, which calls, perhaps, for a different approach with regard to best clinical practice,” he said in an e-mail.
In other words: Just because a 14-year-old girl says she’s a male doesn’t always mean she’s going to feel that way next year. And in fact, Dr. Littman reports that many of these cases resolve within a couple of years
The above is an example of Gish Gallop. Let’s fact check these falsehoods:
Falsehood 1: “Dr. Littman reports that many of these cases resolve within a couple of years.” This seems to be a boldfaced lie. Littman’s own ROGD study shows that 91% of the youth persisted in being trans. Of the 234 individuals whose trans status was known, 213 persisted in being trans while only 3 reasserted a cisgender status. In fact, Littman’s persistence rates are higher than the persistence rates that Dr. Zucker reported: “[I]n adolescence, the most likely outcomes is [the] persistence of the gender dysphoria; 75-80% would continue to have gender dysphoria. The treatment would be [a] social transition and biomedical treatment.”1 Why would Littman tell the press that, “many of these cases resolve within a couple of years” when she MUST know the persistence rate of her own study?
It’s possible that Littman chose to cite outdated DSM-IV Gender Identity Disorder (GID) data instead of current research to support her claim that “many of these cases resolve within a couple of years.” However, old DSM-IV GID and current DSM-5 GD represents different diagnostic populations and conflating the two, thereby misleading the public seems quite unethical.
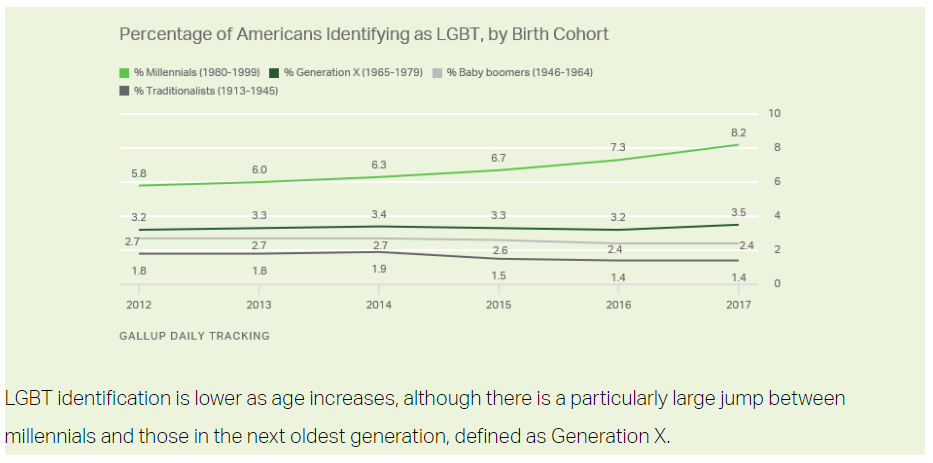
Falsehood 2: There is a “sudden surge” in young girls claiming some type of trans identity. ROGD activists seem to always fail to disclose that twice as many Millennials as GenXers self-identify as LGBT, leading readers to draw the false conclusion that only “young girls” are “suddenly” and increasingly identifying as trans. In other words, all LGBT identities among youth are significantly higher than they were in the past:
Falsehood 3: Young people probably aren’t trans because they’re actually autistic. Consider the following from a 2018 paper published in the Journal of the American Academy of Child & Adolescent Psychiatry:
More recently, growing attention has been paid to a putative relation between gender dysphoria (GD) and autism spectrum disorder (ASD). This concept has become particularly popular in the lay press. Some individuals have gone so far as to suggest that transgender identity is a result of underlying psychopathology, with ASD being one example. These conclusions are not supported by extant research, and practicing child and adolescent psychiatrists should be aware of the literature on this topic and its limitations.
This paper is titled, “Gender Dysphoria” and Autism Spectrum Disorder: Is the Link Real? As this paper correctly notes, the idea that Autism and GD share a link has, “become particularly popular in the lay press.” While it is certainly true that there are trans people with autism in the same way that there are cis and intersex people with autism, the current research does not support the type of causative link ROGD activists like to push, particularly in the media.
Falsehood 4: Young people can be contaminated by non-heteronormative gender. In the 1980s, anti-gay conversion therapists were terribly concerned that non-heteronormative sexuality was a social contagion. These anti-gay activists thought that heterosexual kids could be contaminated by non-heteronormative sexuality through comic books, TV, video games, movies, or other kids who might be gay:
“In the case of homosexuality, it has over the past couple of hundred years been seen both as a disease itself, and as a course of disease, a contagion which, unless contained, will not only lead to the innocent young becoming homosexual, but will cause even worse diseases.”2
ROGD activists have taken up this social contagion rhetoric; consider that Littman claims that cisgender youth can likewise catch transness: “There are examples in the eating disorder and anorexia nervosa literature of how both internalizing symptoms and behaviors have been shared and spread via peer influences which may have relevance to considerations of rapid-onset gender dysphoria.”3 Worse, citing Littman’s ROGD study, the Wall Street Journal recently reported that, “pro-transgender YouTube videos and blogs might have been influential” in cisgender children becoming contaminated with transness.
ROGD isn’t Science
WPATH, the international organization that sets the psychological and medical standards of care for transgender people, recently addressed ROGD. They wrote:
[I]t is both premature and inappropriate to employ official-sounding labels that lead clinicians, community members, and scientists to form absolute conclusions about adolescent gender identity development and the factors that may potentially influence the timing of an adolescent’s declaration as a different gender from birth-assigned sex. [A]ll persons—especially adolescents—are deserving of gender-affirmative evidence-based care that adheres to the latest standards of care and clinical guidelines. WPATH also urges restraint from the use of any term—whether or not formally recognized as a medical entity—to instill fear about the possibility that an adolescent may or may not be transgender with the a priori goal of limiting consideration of all appropriate treatment options in accordance with the aforementioned standards of care and clinical guidelines.
Instead of listening to a researcher-turned-ROGD-activist who seems all too comfortable with lying to the press to further fears about trans kids contaminating cis kids, perhaps consider the scientific consensus as asserted by the American Academy of Pediatrics (AAP)4. What follows are some helpful pointers from AAP:
● When your child discloses his or her identity to you, respond in an affirming, supportive way. Understand that although gender identity is not able to be changed, it often is revealed over time as people discover more about themselves.
● Accept and love your child as they are. Try to understand what they are feeling and experiencing. Even if there are disagreements, they will need your support and validation to develop into healthy teens and adults.
● Stand up for your child when he or she is mistreated. Do not minimize the social pressure or bullying your child may be facing. See How You Can Help Your Child Avoid & Address Bullying.
● Make it clear that slurs or jokes based on gender, gender identity, or sexual orientation are not tolerated. Express your disapproval of these types of jokes or slurs when you encounter them in the community or media.
● Be on the lookout for danger signs that may indicate a need for mental health support such as anxiety, insecurity, depression, low self-esteem, and any emotional problems in your child and others who may not have a source of support otherwise.
● Connect your child with LGBTQ organizations, resources, and events. It is important for them to know they are not alone.
● Celebrate diversity in all forms. Provide access to a variety of books, movies, and materials—including those that positively represent gender diverse individuals. Point out LGBTQ celebrities and role models who stand up for the LGBTQ community, and people in general who demonstrate bravery in the face of social stigma.
● Support your child’s self-expression. Engage in conversations with them around their choices of clothing, jewelry, hairstyle, friends, and room decorations.
● Reach out for education, resources, and support if you feel the need to deepen your own understanding of LGBTQ youth experiences. See Support Resources for Families of Gender Diverse Youth.
After reading the WPATH statement on ROGD, consider reading the following scientific consensus statement from AAP:
If you are curious about what “Affirmative Care” actually means, consider reading The Gender Affirmative Model: An Interdisciplinary Approach to Supporting Transgender and Gender Expansive Children from the American Psychological Association.
- Zinck, S., & Pignatiello, A. (2015). External Review of the Gender Identity Clinic of the Child, Youth and Family Services in the Underserved Populations Program at the Centre for Addiction and Mental Health. Toronto: CAMH.
- Adler, M. (1988). Diseases in the Homosexual Male. New York: Springer-Verlag.
- Littman, L. (2018). Rapid-onset gender dysphoria in adolescents and young adults: A study of parental reports. PLOS One.
- Not to be confused with the anti-LGBT hate group that apparently pretends to be AAP.


