
By Kelly Winters, PhD
Jesse Singal, the Senior Editor at nymag.com, has enlisted his New York Magazine blog to promote the widely publicized presumption that painful distress with birth-assigned sex and gender are just a phase for the great majority of children who suffer it:
While the actual percentages vary from study to study, overall, it appears that about 80 percent of kids with gender dysphoria end up feeling okay, in the long run, with the bodies they were born into.
Singal’s article defines “desistance” as, “the tendency for gender dysphoria to resolve itself as a child gets older and older.” Singal praised the 80% “desistance” claim in his article as “solid scientific consensus” and boasted that “every” study, not some, but “every study that has been conducted on this has found the same thing.” He scorned those who do not accept the 80% presumption (Tannehill 2016, Serano 2016, Olson and Durwood 2016) as “part of the problem,” as essentially “ignoring” science, and preventing “intelligent, informed discussion.”
The real problem, however, is that Singal’s support for the 80% presumption and its promoters from the Toronto Clarke Institute/Centre for Addiction and Mental Health (CAMH) and the Dutch VU University Medical Center rests on a critical, misleading statement in this article:
It’s hard to imagine a kid meeting all the necessary criteria in the DSM-IV and not ‘actually’ being gender dysphoric… Since 63 percent of the subjects in Singh’s study met these criteria, this really wasn’t a sample of children who were ‘just’ gender nonconforming.
The author preceded these remarks with a listing of the 1994 Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV)[1] diagnostic criteria for “Gender Identity Disorder of Children” (GIDC, 302.6) that were used for intake selection in childhood “desistance” studies in Toronto and Amsterdam between 1994 and 2013, but the actual diagnostic criteria contradicted his conclusion. In fact, the subcommittee responsible for Gender Identity Disorders in the DSM-IV, as the 4th edition is known, deliberately chose to allow diagnosis of GIDC without any “explicit wish to be of the opposite sex”[2] –a loophole that was partially corrected in the DSM-5, published in 2013. For example, the following statement could be false, and yet children could still be diagnosed as having a “gender identity disorder” under the DSM criteria used for “desistance” research:
“1. Repeatedly stated desire to be, or insistence that he or she is, the other sex.”
The above quote comes from Subcriterion 1 of Criterion A of the Gender Identity Disorder of Childhood diagnosis, but this subcriterion was not required for diagnosis. In fact, only four of five subcriteria were required to meet Criterion A. Here are the remaining four. They all describe gender nonconforming behavior:
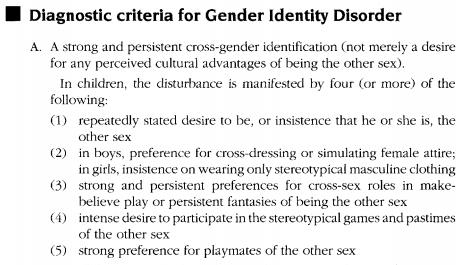
By this now void standard, children could be judged to meet Criterion A strictly on the basis of gender nonconformity alone, with no indication of actual gender dysphoria or incongruent gender identity. Here’s a quick breakdown of the rest of the now void DSM-IV and DSM-IV-TR criteria :
Criterion B referenced gender dysphoria (in the Fisk, 1973, sense of distress with physical sex characteristics or assigned gender roles[3]) but once again had loopholes that allowed diagnosis because of behavioral gender nonconformity without evidence of actual gender dysphoria. Birth-assigned boys could meet criterion B with “aversion toward rough-and-tumble play and rejection of male stereotypical toys, games, and activities.” So could birth-assigned girls with a “marked aversion toward normative female clothing.”
Criterion C excluded diagnosis for children with intersex conditions.
Criterion D was the clinical significance criterion, added to almost all categories in the DSM-IV. It required significant distress or impairment in “social, occupational, or other important areas of functioning.” However, the GIDC supporting text maintained that distress from societal prejudice, rather than from gender dysphoria itself, would meet criterion D (APA 2000, p. 577).
To be clear, the criteria of the DSM-IV –the very standard under which kids could be diagnosed with “gender identity disorder” without actually having gender dysphoria– is how these researchers came to tout an 80% desistance rate that is quoted in New York magazine. Remember, these flawed standards[4], [5] are NOW VOID. These loopholes were partially corrected in the DSM-5 in 2013, but the data from the prior “desistance” studies of gender nonconforming children were never reevaluated in light of the new diagnostic criteria.
The 80% “desistance” myth is like claiming that since most mammals don’t have spots, leopard cubs are most likely to “desist” in being spotted. That’s not science. That’s not logic. That’s something else entirely. The conflation of a much larger superset of gender nonconforming children, who never actually suffer gender dysphoria, with a much smaller subset of children with actual gender dysphoria is not “solid scientific consensus.” Gender nonconformity is not gender dysphoria. Children who were never gender dysphoric to begin with are not “desistant.”
Watch the Video Version of this Essay
A version of this article originally appeared on GID Reform.
- American Psychiatric Association (2000). Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision. Washington, D.C.
- S. Bradley, Ray Blanchard, et al. (1991). Interim Report of the DSM-IV Subcommittee on Gender Identity Disorder Archives of Sexual Behavior, Vol. 20, 4, p. 339.
- Fisk, N. (1973). Gender dysphoria syndrome. (The how, what, and why of a disease). In D. Laub & P. Gandy (Eds.), Proceedings of the second interdisciplinary symposium on gender dysphoria syndrome (pp. 7–14). Palo Alto, CA: Stanford University Press.
- Winters, K. (2008). Disallowed Identities, Disaffirmed Childhood. GID Reform Blog: Issues on reform of the diagnostic categories of Gender Identity Disorder and Transvestic Fetishism in the DSM-5, Oct. 28. https://gidreform.wordpress.com/2008/10/28/disordered-identities-disaffirmed-childhood/
- Winters, K. (2014). Methodological Questions in Childhood Gender Identity ‘Desistence’ Research. 23rd World Professional Association for Transgender Health Biennial Symposium, Feb. 16, 2014, Bangkok, Thailand. https://gidreform.wordpress.com/2014/02/25/methodological-questions-in-childhood-gender-identity-desistence-research/


A study in Australia found the rate to be 4%
That is more or less consistent with other studies.
Unfortunately, many people who transition find out that the process did not solve any other mental health issues they might have had. That is the problem. Parents and gender specialists are quick to declare a child trans without any discussion with the child to find out why they feel that way.
wrong, those are the hate filled talking points less than 1 in 20 transition and regret because they were NOT trans, and that figure was before the standards were made harder, so it is less now. some regret after because the surgeon botchs the surgery, generally that is it, all the ones i know otherwise are all older who were treated under the old standards.
Nice try though, but big fail
I think you would consider any criticism a big fail. The kind of reaction I would expect from a man who considers all women as inferior beings.
LMAO yep definitely a Terf here. i look at all real criticisms not the quack stuff you and your ilk quote, i use the medically peer reviewed studies, things that over 95% of the worlds medical establishment follows, not the quack stuff you are spouting from your fake profile
Anyone citing the 80% study are Transphobes. The 80% study never met any standards required of a proper study, and that is documented. When Ray Blanchard is quoted, it shows you are completely ignorant of anyone being Transgender. NY Times is no longer checking articles for being truthful and honest, as this article shows.
so now after transitioning, you say you were wrong, but you havent gone BACK, why is that mark? or your wife? interesting questions dont you think.
We arecywp spirited expressing hormone free and teaching people the truth.
Going back? I never went anywhere that is what I finally realized, transition is a farce and I love how you cannot engage in conversation on your page and lie about me, I have never once tried to contact you, you are the one that writes on these comments, I kindly shared a video with you so you can see the affects of synthetics, yet you blocked and removed the video. I am a woman, I no longer Identify as a man, but the use of Testosterone creates secondary affects, you know the ones you can’t get rid off. I am a woman no matter what I look like, you can’t say the same.
oh if it isnt the anti trans, trans man, him and his wife transition, then its NOT real, lol. go away little person.
Yeah man, trans advocates that realize this whole thing is a lie, big pharma lab rats. A man will always be a man and you are ugly. Stop while you can.
awww did i hurt your feelings, better than the kids you kill with your crap.
lol, you don’t have that kind of power, I save kids, you kill them with life long drugs and surgical procedures.
all they have to do is take a look at you, and know that they would never want to be like you.
LOL thats all you can say, is i am ugly? at least i am a caring person, not someone pedaling their crap like you and mark, to vulnerable kids and parents who are looking for a reason NOT to help their kids. go sell you snake oil crap on amazon or ebay
please name ONE real advocate that has done this. and cite PROOF
oh look its everyones UNfavorite anti trans trans man.
not a trans man, I am a female, as you are a man
wow, male name you present male, so what you cant give up the male privilege i guess? your a fraud and dangerous
its my legal name, I am the fraud? LOL, you are the one lying about your gender, and not really lying, because people can see a mile away that you are a man with real male privilege. I was socialized as a woman, don’t know how to use male privilege, but you do.
lol, yeah not so much fraud. this is my legal name too but ONLY YOU get that exemption huh? nice…. NOT. your just a fraud who cant fully admit it. you could easily change back, stop taking the T, change your name back, only thing that would is the voice and some extra hair growth. so you CHOSE to be this way, you are a FRAUD.
what exemption, I am not exempt from anything, I identify as a woman. A fraud, I am not the one claiming the sex that does not belong or fit. I have stopped taking T, and I am just a woman with lots of facial and body hair. why should I pay the courts money to change my name, why should I fall for the stereotypes?
and why do you have to keep making new profiles, i have blocked you i dont know how many times.
you lie, you blocked my mark angelo cummings profile, that is the only time, why do trans women lie so much? Oh wait, thats because they are living a lie. You responded to my comment here to someone else and as a nosy nily, you had to intervene. So what is your point, you have nothing.
just an AGP living a lie.
Yeah, you should probably check this out before engaging Mark:
https://soundcloud.com/cristan-williams/quislings-mark-lynna-talk-with-bugbrennan
Mark seems to think labeling people on the internet will make them happy or lead them to truth. It’s useless to discuss material conditions with them because they can’t seem to grasp materialist analysis and consistently confuses their reductive essentialist rhetoric with material bodies and their material conditions.
Yes, i know, i didnt realize it was him until i watched the video link, as i said i have blocked him many times before as being a pest. now he is using TWO profiles
Yeah, they were previously banned from the TransAdvocate for trolling. Aparently they got a new account to circumvent their ban.
you are falling for the stereotype and lies, gender is a fallacy.
you are an idiot, as i stated. yes there are those who use FAKE numbers, or faulty studies, we have REAL science, peer reviewed, etc.
fine YOU werent, that does NOT mean the rest of us are fooling anyone. yes i am trans and knew when i was 5.
Real science? No sorry there are none. Its all subjective. Yes you and everyone who claim they are trans.
yes all the brain dissections, MRI’s Sonograms, etc are all fake, got you. and the earth is flat too right
are you mark cummings wife, husband, whatever? i dont know since if you are you look female say you identify as male as your birth sex, etc, but refuse to make yourself look male, sounds like YOU are the confused pair here, not everyone else
no this is Mark, Maritza is my female name. I was born a bio female, I transitioned in 2003 and detrans in 2015, we are not confused, on the contrary, we got it right now.
but you continue to be confused
Even if you dispute the 80% number, you need to admit that most children will go onto to admit their birth sex, and be heterosexual or homosexual after going through a normal puberty.
yeah, no. the 80% number is NOT just trans kids, they put ANYONE who had a “gender non conforming” activity/etc in the mix. so tom girls, boys are just a bit feminine seeming, etc. its CRAP science made to fit the answer THEY wanted. same kind of crap science most the doctors, etc who say its not real use. some trans are homosexual, most are straight, might be a slightly higher incident of being gay, from being forced to “conform” to societies standards.
By the way, you have free will. You can still be considered a male or female even if you don’t conform to societal expectations. That’s how we got tomboys and effeminate boys in the past.
and yet you keep ignoring the reasons why that is NOT what we are, so i call you TERF, for your other statement shows that is WHAT you are.
Libertarian free will is nonsense. Anyone asserting it as part of their gender analysis is someone who’s so lost to their logical confusion they don’t… can’t know they’re lost.
Even Dr. Zucker asserts that most gender dysphoric kids DO persist in having gender dysphoria. The 80% number comes from a MIXED group of gender dysphoric AND gender nonconforming kids. Of that MIXED group of mostly gender nonconforming kids, most of that group will not have gender dysphoria.
Even if the numbers are true and there are 80% desistors does that necessarily mean, that the other 20% of persistors are invalid? And that the latter should be forced to desist?
Wow, it’s because of study’s like these and often tilted media articles that I decided to publish our family’s journey to discovering the son we never knew we had. My son, is now a health, happy, well adjusted 18 year old transgender man and trying to conform to society’s binary almost killed him in his teens – thank goodness we didn’t believe he’d grow out of it. If we had of held that mentality and forced him to stay on the path to wait for him to feel ok, he likely would be dead today. Kindest regards, Cheryl B. Evans
Anytime someone writes using the ” 80% ” study, it is a false study incomplete of documentable information.
So glad that you have made clear the problem with the diagnostic criteria used in the much quoted studies. There are a few more points though.
Singal mis-stated in his article that the diagnosis used, and quoted was Gender Dysphoria – the current diagnosis. How many mistakes can he make before we call “prejudice”?
Recent research on how the “desisted” former patients of children’s gender clinics differed from those who “persisted” found that most “desisters” said that thy found they were happy with what their physical sex enabled after puberty started, whereas the “persisters” became increasingly unhappy with their physical sex – an opposite reaction to pubertal hormones. In terms of what indications there might have been before puberty, it was generally “the earlier and most intensely dysphoric” who persisted. Thus Singal’s gloss that “desisters” had “rather severe gender dysphoria” is even more misleading.
This ignoring that the most dysphoric (or perhaps the only ones who actually were dysphoric, as opposed to gender-non-conforming) are the ones who need the right puberty – medical transition – has been deliberate and of long standing. Peggy Cohen-Kettenis is on film saying in 1995 that the children who reject the sex of their body, or demand that of the other sex, never change their minds. She was then head of the Netherlands Children’s Gender Clinic, and leading in providing hormones at 16 rather than denying them until 18. Unfortunately she hasn’t advanced her ideas much more since then. The head of the HBIDGA, then WPATH Children’s Committee for many years was head of the London children’s clinic, which has long been allied with Kenneth Zucker. From their founding in 1989 until only about 2 years ago they were citing desistance, and being quite unable to tell which patients needed medical intervention, to deny medical intervention to all patients. Their records were audited for a paper published in the IJT and it was found they had no records of which patients expressed physical dysphoria, and therefore the records were not there to back their desistance findings. That was probably often the case. Clinics were avoiding being of assistance; instead children, and their families suffered greatly.
I wrote quite a bit on this https://medium.com/@oatc/in-detransition-desistance-and-disinformation-a-guide-for-understanding-transgender-children-5ea27284445c?source=responses———0- in response to Julia Serano’s piece on the same site.
As a woman who was a trans child – coming out as a girl at 30 months – and whose parents were forced to follow the prevailing advice that desistance should be encouraged, this matters greatly.
yeah this is complete crap. the 80% figure is when its kids going “through a phase” like tom girls, etc, and grow out of it. not the same thing. i hate people who twist things to fit their goal/agenda.
Like you trans and supporters don’t do the same thing?
LOL, yes. look who ever you are, you dont know MY story, and if you did, you would likely be crying and apologizing. i knew when i was 5, when i first noticed my younger sister was different than i was. for several years i told everyone in my family, was told its just phase, etc, etc. until between 8-9 three cousins used it to get me to be “compliant” by treating me like a girl, said they believed me, etc. and proceeded to “teach” me how a girl acts for a boy, for over a year. after this happened and i figured out it was bad/wrong, i blocked it for the next 30+ years. i always had compulsions about girls, not liking them but liking what they wore, more friends were girls etc, i figured i was a cross dresser, it was the 80’s transsexuals were all but unheard of in most parts of america. then for a while i thought i might be gay. after several failed attempts at relationships, i gave up, and focused on helping my sister and brothers families, then cared for my mother for the last 10 years of her life. it was ONLY after she passed, and at her memorial i learned that one of my molesters was in prison for doing it to HIS three sons, one was dead, the other was living scott free in Oregon. this caused a recall of what happened, and over the next 9 months i was fighting guilt and grief about my mothers death, the memories i was recalling. finally the depression was so deep and after much research on the internet, i finally went to therapy, it took most of a year for ME to admit i was trans (no the therapist was NOT pushing it, she was NOT a gender specialist, but someone who had personal experience, cousin, child of a friend, etc) because i was worried what was done to me may be influencing my memories, but it wasnt.
see a lot of trans are prime candidates for pedophiles, who is going to believe the little boy who says hes a girl when he is trying to say good uncle joe was doing naughty things to him? he OBVIOUSLY is just making it up, right?
as to the research, no, many scientists, NOT involved (its called PEER review) saw that the numbers were being manipulated by adding in people who should NOT have been included.
You were born male or female according to your body parts. Not acting to social or family expectations does NOT make you transgender. Why did you even think your ‘gender identity’ had to match your birth sex in the first place? Do you think most of us normal people even think about gender presentation on a daily basis? We don’t.
how stupid are you? thats kind of the whole freaking point. when your gender IDENTITY and you physical body do NOT MATCH, that is the very definition of being transgender/transsexual. everyone thought i was going to be a girl i came out with some male anatomy. i never knew this until my mother passed away (that they thought i was supposed to be a girl, in 69/70 it was not as accurate as it is today) i dont have the money to do genetic tests, i already know i have genetic issues from birth.
here is something to look up, by your unintelligent thinking, anyone with XY is male right? or XX female? there are members of both sexs who have the OPPOSING set of chromosomes, or have extra, or missing one. xy/xx are the Average/majority, they are NOT the SOLE and ONLY way sex is defined, not for a a decade or two, but when you listen to people teaching 80 year old science, what can you expect?
as to why i “ever thought that” i didnt, until i saw my baby sister and saw the differences. even at five i wasnt like my brothers, i knew it hell m y whole family knew it, they just didnt know what to make of it. my mother thought it was her fault as a single parent, so forced me to do tee ball and little league. i did it to please her, not for myself. you had no issue so you didnt have to “think about it” thats the “privilege” of a CIS person, they dont have to go through what we do.
i have yet to meet more than a few trans people who if offered a 100% sure fire fix for being this way who woudnt take it. whether it was one way or the other. its not about WANTING to be one or the other, its about BEING that. and since they have NO fix for the brain yet, the ONLY effective treatment is for what is going on now, Therapy, HRT and for some, SRS/GCS. but not all can or need to go that route. some can live as they are and prefer NOT to risk surgery. some have self mutilated themselves to get rid of their deformity (which is dumb because without that tissue, a functioning vagina can NOT be constructed with todays medical knowledge.) so you can think what you want, but someone who cant even show their face or a real profile is pretty much a coward and/or troll in my book
Why did you feel that your gender identity ( other than the stereotypes expected of your sex) had to match your birth sex? As for the rest I am older and actually like my privacy. I am not a millennial who lives on social media like Facebook.
ok, i am assuming you are female based on the name, how would you feel if you woke up with no breasts and a penis tomorrow? most of us DONT realize until later, but some realize sooner. one of the KEY things that Therapists look for is that anyone claiming to be transsexual/transgender (they are not always interchangeable but a lot of people see them that way) must be INSISTENT, PERSISTENT & CONSISTENT not for weeks or months but years. it is why there is a protocol to prevent those who are NOT but just “in a phase” getting medical treatment that is NOT appropriate. i love how conservatives think its either about getting attention (the kind of attention we get is NOT the kind most people want, being bullied, discriminated against, beaten and oh yeah MURDERED just for the fact we are transsexual, yep everyone wants that kind of attention) or that doctors/therapists/parents are “pushing” an “agenda” the only trans agenda i know of is being accepted (i could care less about approval, its MY life, not yours so you should have NO say over how I live it, etc) not discriminated against, etc.
the fact that our gender Identities do NOT match our physical sex causes Gender Dysphoria, this is a condition that can cause mild to extreme stress, depression, etc so while it is NOT a mental disorder/disease, it can cause them, so much so that some have committed suicide, self harmed, or joined groups like the military, police, fire departments in the hopes it would “fix” them and prove they were the man they appear to be, or that the job will kill them and their problem is solved either way. i am sure some join because of a true desire to serve, etc. but the fact a higher than the average percentage join these groups is kind of telling.
i dont live on facebook, but its a good way to contact those who are afraid for themselves and DONT come outside in fear of their lives, or being beaten, etc. its also a good way to do research and so on. but THIS isnt face book its a trans advocacy page that you are trolling. but i will give you the benefit of the doubt and say you TRULY want to be educated on this, is that so? or was my trolling diagnosis correct?
My current questions are about why most people would think their gender identities have to match their birth sex. I grew up before this gender crap, and this whole transgender movement seems to be based on the wrong imo opinion that there is one box labeled male and another labeled female. Within those boxes are strict guidelines about what colors you’re supposed to like, clothes you are supposed to dress in, toys (where applicable) you’re supposed to play with …. Why there is such a need to genderize everything? And why do children have to declare themselves as male or female so young?What good is there in going online when all you hear and read is in the echo chamber of the translobby, backed up by ‘research’ it has paid for. Do you ever think of getting an objective opinion of your condition? Or are you looking for affirmation?
ok i will try ONE more time, using small words.
you NEVER QUESTIONED it because you are “CIS” gender, your physical sex and gender identity MATCH, there is NO dysphoria. this is NOT about colors, or clothes, or toys those are OUTWARD signs used by our society to denote your role, NOT necessarily gender (although they usually line up) not 100 years ago, one of our presidents, FDR, when HE was a child it was the opposite. blue was for GIRLS because it was the “softer” color, Red was for boys. most children up to a certain age wore DRESSING GOWNS, no matter the sex./gender. the issue comes in when other girls are playing with dolls and this “boy” wants to also, but boys CANT play with dolls, its just not done (also these things are GENERALLY based on preferences of the different sex’s of children. girls, whether its influenced by mom, want “babies” to care, for etc)
They DONT have to in most cases, the ONLY time its an issue IS for Trans kids, they are being treated differently than those they who are their peers, and they want the SAME treatment. and the earlier it happens the HEALTHIER, in both body and mind, the child IS.
LOL you have GOT to be kidding me, right? this article alone shows its NOT just the “trans lobby” online, much less an echo chamber. the fact we have SCIENTIFIC, peer reviewed, duplicated, research show that what we are IS validated, sorry if you disagree. saying WE paid for it lol. trans are in the majority lower income because its hard to find and keep a job when you present female but your documents show male. its getting easier, but still hard to GET jobs especially in the climate of HATE fostered by the current republichristian party. there are some are are middle class, even some wealthy ones, but they usually dont transition until later in life.
as to an “objective opinion” i went to a therapist, NOT a gender specialist, but a PhD trained therapist, i went in after i recalled all the things from my childhood i had blocked out, i sent a FOUR page document listing everything i remembered, felt, etc. with the simple subject line of “Can you help”
i have been in her care for almost 5 years now, it took ME over 9 months to accept what i remembered was real, she felt it at around 4 months but DIDNT SAY ANYTHING. she did her JOB, not fulfilling a quota, or working to write a book, etc. are there some therapists out there like this? sure we know they are because there HAVE been some (supposedly at least) who claim they were “convinced” by their therapist. which isnt how therapy normally works, they guide you to asking the RIGHT QUESTIONS at the most, get what YOU think, etc. yes they exist, but are probably less than 1% of those practicing. most therapists do it to HELP people, not make them into something they are not.
you are cis too, just confused.
so you are living a lie then? you transitioned, but NEVER detranstitioned, but expect everyone ELSE TOO????? self deluding person your are, yes?
no one transitons anywhere where did you think you went to, you are still you, just with a wig and make up. I did detransition, no longer take hormones or identify as a trans anything.
Must have been tough to de-transition. I’ve read stories about trans who de-transitioned, and are suffering medical issues plus losing many friends who abandoned them when they did.
no because they DIDNT detransition. they still appear as their assumed gender, NOT their birth gender, still use those identities, etc. that is NOT detransitioning, if they did, they would re-assume their birth gender roles, neither one has. although Mark/Marizta use both so they can trash people twice as much.
I grew up in a traditional Chinese family. Your ideas about gender identity is alien to me.
so why are you saying what your saying in earlier posts? if you DONT know or understand, would it have NOT been simpler to ask before stating boy is boy, girl is girl?
No. I expect a person’s body parts to match their outward appearance. I don’t place any special emphasis on gender identity. I am a woman because I was born with the corresponding body parts, not gender identity.
here is another thing for you to think about. you do agree that intersex (used to be called hermaphrodites, having some of both sex’s genitals to one degree or another) are real, right? its kind of obvious, they have PHYSICAL signs.
one of the leading theories is that transsexuals are PART of the intersex spectrum, just that the “confusion” in the womb is less on primarily effects the brain development early on rather than later when physical changes are supposed to happen. yes its a THEORY with some evidence, just not conclusive. a lot of intersex are operated on not long after birth to “fix” their bodies. the way it goes varies, what the doctor recommends, the parents preference, etc, the ONLY thing they DONT, and cant, take into consideration is the GENDER identity of the intersex child, so a lot of them are “transsexuals” because in the past, it was a “bad” thing to have an intersex child, it was demeaning etc, so for the “childs” mental health, a lot of times the surgery is HIDDEN in their files, listed as “minor corrective surgery” or some other innocuous thing. i have a friend who went in for her pre surgery check up before getting SRS/GCS surgery, and they found (and she is in her 40’s) a WORKING Fallopian tube and uterus in the ultrasound. she had always had bad cramps/stomach aches, some bleeding in her urine, but they never found a cause, it was because she was having periods and because her condition was NOT listed in her files, her later doctors NEVER EVEN LOOKED into this, because it is pretty rare.
i am not saying that being transgender or intersex is “normal” but it is NATURAL, it is a variation, just like you have albino’s, or a blonde kid with generations of brunettes, etc. anytime someone has something out of the ordinary it is usually caused by a genetic variation. the cause of the variation is what they are trying to find. some are linked to some drugs in the sixties (this caused a variation that has lasted for 4 generations now, so likely permanent in that families genome) or just genetic Lottery. i was born with several genetic issues, no working immune system for the first 18 months, with it had bad lungs, colitis for my whole life, etc.
Nope intersex people want their movement back, and don’t appreciate you trans using their arguments for your situation. As for the science, research has been bought and paid for by the translobby. Many scientists fear for their incomes and research funding. That is why you won’t hear from them.
“intersex people want their movement back” said every sex essentialist activist who’s never taken the time to sit down with an Intersex person over coffee and get to know them. How much IRL material support have you given to Intersex causes and actions? Even better, name a TERF org that has Intersex people have leadership positions.
The reality is that sex essentialist activists USE Intersex bodies as rhetorical tools and nothing else. You don’t get to speak for our Intersex members, especially those who sit on our Board of Directors. You don’t speak for Intersex activists from groups like THIS (who got the first Intersex bill considered in the South) or Oii-America. I bet you don’t even know why Intersex Awareness Day is on the day it is (hint: it has to do with trans activists).
Intersex bodies are not your rhetorical tools. You don’t get to speak for our members who are Intersex activists. You only get to speak for a group of sex essentialists who are chasing a ghost of empowerment by trying to control the labels trans and Intersex women use when describing their material condition.
Why not read what an actual Intersex person has to say about your crew’s sex essentialism and the talking points you’ve just regurgitated here: http://www.transadvocate.com/an-intersex-perspective-on-the-trans-intersex-and-terf-communities_n_14539.htm
The current THEORY is that transsexuals are a from of intersex, just as they have varying degrees, one of the prevalent theories is that while our outward appearance is fully of one sex, the brain has developed another. so they are thinking that AFTER the brain started developing but before the body made sex changes it changed directions, vs in the middle of the primary/secondary characteristics being changed to one sex or the other, creating the intersex condition VISIBLY identifiable, where if ours are “fully complete” in one direction, they cant see the issue until WE can point it out. it IS just a theory, but one supported by some research better than the twaddle Mark is peddling
the body and the brain are one in the same, look in the mirror please stop lying to yourself.
Still not a woman.
yep terf troll thanks for proving it.
No. I’m a private person. I am not on social media like Twitter, Facebook etc because I have a life aside from social media. You know what happens to people who reveal too much? They get harassed and bullied. Besides, I have the right to my boundaries, and I don’t need to reveal my personal details to every Tom, Dick and Harriet out there. You have no more right to my personal details than I have to yours.
also, most of us want NO ONE ELSE to have to go through this, you tend to think its about attention? yeah the highest death rate per capita of ANY other group, great attention. until very recently most of us could not get work, housing, etc (when you look and act female but your id shows male, its really easy to discriminate) we get assaulted, both verbally, physically and sexually at a higher rate (after all, thats all tranny’s are good for right, sex? or so the cretin thinking runs)
Sorry (not sorry) but I don’t participate in Oppression Games. Way to put your special needs above any born woman who has had to put up with sexist crap since the day she was born.
lol, yes facts are so inconvenient arent they, its fact that more trans women are killed, percentage wise of their demographic than any other. we dont have special needs, just simple accommodations. thanks for proving your a TERF or similar anti trans person though.
Still playing victim. Do you think you will ever get past the idea that you are the most victimized group on earth? Us born women face obstacles from the day we are born that you will never face. Also convenient of you to ignore the hundreds of born women who are killed every day around the world.
lol, again putting words in my mouth. i never said that, but i do stand by what i said. i never said that women should be ingored for dying, again you show your being a terf or their like. if you want to give me PEER REVIEWED scientific studies, i will look at them i spent over 2 years looking at things after i recalled what happened to me to figure out WHAT i was. but this will be the last response, tired of feeding the fake profile trolls.
i am so glad YOU KNOW that i was never treated badly from birth (i wasnt until 5, nor are most children even girls, now who is playing the victim. maybe in your sick culture its common, but not here, it happens, but is NOT common) or at 5 when i tried to tell my family who i really was, or at 8ish when 3 cousins used that knowledge to get me to comply with their perverted desires for over a year, and upon realizing what was happening was wrong, i didnt repress those memories for over 30 years, never fitting in because i never felt right, and couldnt even remember WHY, nope not at all.
Then you should have been seeking pyschological help.
you are very ignorant, any real transsexual IS under counseling, its the only RIGHT way to get HRT and SRS. just goes to show you “gender critical” morons cant even look up your facts before trying to put someone down.
If you don’t know the difference between material reality and your thoughts about material reality, you’re making something like a POMO argument. The material condition of cis women defines the material condition of trans and intersex women, not your thoughts about essentialist reductionism.
Sorry, your thoughts about words and their meaning do not construct the material realities of body phenotype or material conditions within society. It might make you feel empowered to make your POMO pronouncements, but you controlling the labels Teresa uses to describe her material condition won’t make you free.
You as a transwoman has a superficial idea of what a born female’s life could be like. Forced marriage, sex slavery, female genital mutilation, being killed or aborted because you are born a female, etc. Your insistence on the supremacy of gender identity over sex identity will only take away from women’s rights fought over centuries. Or maybe, that is your goal? To destroy women’s rights to prove your male supremacy? That makes you no better than the MRAs.
You wrote: “Forced marriage, sex slavery, female genital mutilation, being killed or aborted because you are born a female, etc.”
Are you saying that you’ve experienced these things and are therefore female?
No. I am saying those things would only apply to born females not born males who identify as female.
I take it you’ve never visited East Asia?
May Loo asserted that sexual slavery only applies to “to born females not born males who identify as female.”
http://www.cnn.com/2017/01/02/americas/transgender-san-jose-costa-rica/index.html
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4204396/
http://news.trust.org/item/20170425040745-h56o1/
“Transgender people are highly discriminated in their access to employment and severely ostracized due to their gender identity. This risk of marginalisation impacts on their vulnerability to engage in prostitution as the only option available. Studies show that transgender prostitutes (male to female) experience the same frequency of violence as “cisgendered” women.” – European Parliament’s Committee on Women’s Rights and Gender Equality, 2014
“Governments and NGOs have made progress in identifying LGBT trafficking victims and highlighting the vulnerability of LGBT persons to crimes such as human trafficking. For example, in 2013, NGOs working on LGBT issues in Argentina identified traffickers who promised transgender women job opportunities in Europe, but instead confiscated their passports and forced them into prostitution. ” – US State Department, 2014
One thing that bothers me. Why do you trans go after terfs or gender critical feminists like myself online and elsewhere when it is men who commit crimes like murder against you? You’re a born male. Have you ever challenged men on what they do?
If you mean why do I call out TERF behavior and document past IRL violence? I do it to counter fallacious essentialism, document the material harm their movement has done, and to hold up the pre-disco era radical feminism that was trans-inclusive prior to TERFs using violence against trans inclusive radical feminists in their effort to colonize radical feminism.
The pioneering radical feminist org, the Olivia Collective was trans inclusive & your movement threatened to kill them. Then you threatened to murder Sandy Stone before you showed up at an Olivia event, armed with guns, to do just that.
The militant radical feminist org, Cell 16 was trans inclusive before TERFs colonized the group, forcing out the trans-inclusive radical feminist founders.
What about that time TERF began beating trans-inclusive radical feminists like Robin Tyler at the West Coast Lesbian Conference in their violent attempt to purge trans women from the event, even though it was organized through the trans-inclusive radical feminist organization, the Lesbian Tide Collective?
That’s to say nothing of TERF political activism resulting in the revocation of trans health care.
You are part of a decades-old anti-radfem group that presents itself as radical feminism itself to those who don’t know the history. You probably won’t know about when your group threatened members of the Lesbian Avengers with a knife for being trans inclusive because you don’t know your group’s history.
This is the bloody history you serve, not me.
The women’s movement was about advancing the rights of born women, not men thinking themselves as women like you. As for the rest, you insist on blaming the entire movement for the actions of some women decades ago. Also, you are being American-centric. The women’s movement wasn’t just in the US. It was all over the world over centuries. Women elsewhere were fighting to just exist – not the right to be accepted as female.
Please go read Right Wing Women by Andrea Dworkin, ML.
Ironically I am not your typical conservative. You like to generalize the opposition as bible-thumping right-wing whackos. There are people on the left and right who are rightfully concerned about your movement. Entitled man that you were, you still believe that you have the right to redefine the term female to the rest of us. You don’t. It is a dictionary definition, and you can’t just ‘self-identify your way into womanhood.
lol, yes we know there are people on all sides of the political spectrum who are against us being who we are, gay men who thing we are just afraid to admit we are gay men, you know because it is SOOOO much harder to be gay than trans these days. people like you, feminists, straight and gay (THESE are what a TERF is what you have proven to be) lol yes i was so entitled growing up, on welfare, not able to go to college because having to work caused my grades to slip, even with high sat scores. yes that white male privilege sure worked for me, NOT. because i was NEVER MALE, i may have been faking it most of my life, but most could see that, some just figured i was gay, etc.
yes because Dictionary definitions are NEVER changed, dont be so stupid. as to “self identifying” we dont, we can claim it but in order to LEGALLY be who we are, we have to PROVE it to therapists, two of them, live as we want for a period, etc.
Did I say you were a right winger? Nope. I encouraged you to read Right Wing Women by Dworkin.
You seem to believe that the material condition of women is defined by a dictionary. Is that correct? Or, are you saying that “woman” is something other than her material condition?
You should read up on the long list of transwomen who have committed brutal crimes as well. Don’t make it sound like it’s all one-sided.
Yeah, and I can google cis women sex abusers right now and come up with a list a mile long. You asked me why I ‘go after TERFs’ and I told you that exposing the violent history of TERFs was important. You claiming that out of all history the world over, there happens to be some trans women who’ve committed crimes is irrelevant.
Show me a trans activist that showed up at a TERF event with guns because they announced their intention to murder a specific TERF. YOUR group did that to trans-inclusive radical feminists because they had trans members. That’s YOUR history, not mine.
Show me a trans activist who threatened the Lesbian Avengers with a knife. YOUr group did that to the Lesbian Avengers because they were trans-inclusive. That’s YOUR history, not mine.
because TERF’s/WoLF’s and “gender critical feminists” like you do as much damage, just on a wider scale, and generally not physical. your kind of claims are what feed into the hysteria that HELPS make a man into a killer of trans women.
it was a TERF who has done the most damage, Janice Raymond, who was responsible for REMOVING SRS from the standard of care in the US, the Carter admin commissioned a study, SHE did that study, using the same crap as listed above, and the government declared SRS “experimental” which allowed every insurance carrier to NOT cover it, since the early 80s, so all trans suicide based on that lays SOLELY on her doorstep, of course she is PROUD that her work KILLED trans who most of you dont consider real people anyway. it was proven JUST LAST year when a trans woman fought the findings of that “study” and all the medical personal in the review board agreed it was a false study, using bad information.
Born men kill transwomen yet you insist on blaming us born women for those crimes. Besides do you believe that any born man who commits crimes against a transwoman reads any gender critical comments? Who is out there to protect us born women? You wannabes hate us because we won’t validate you, conservatives deny us our reproductive rights, and liberal men are hopeless lapdogs willing to do everything the translobby wants them to and trying to erase our hard-fought rights. And you don’t think we have a right to fight back? You must really hate women despite your insistence on being one of us. Also, you conveniently ignore all the crimes that transwomen have committed. Do the names Dana Rivers, Donna Perry ring a bell?
no one is ignoring it, just like i am NOT ignoring the role YOU and those like you PLAY in this, thats the problem, you dont like being put in the spotlight as part of the problem
and i am NOT ignoring any illegal activity. if they commit a crime they should be punished. IF. i dont hate women, i hate people LIKE YOU who preach hate against something that they think threatens them. Please tell me where this all powerful trans lobby is, because they sure seem ineffective in getting any real things done
May Loo seems to think that trans persons are NOT forced into sexual slavery. we have been forced into several forms, here and abroad. in most terfs views, we are “mutilated men” so yes in their view we know genital mutilation. shes not very bright is she? we are killed for the simple fact we are TRANS and people like her promote the hate and fear, she is batting near zero on her claims. forced marriage? if a trans woman was Post op, in certain countries it could happen, if they are just grabbing people of the street, of course it could happen. and abortion is an equal opportunity killer, while in some countries, they might abort based on sex, its not very common, killed after birth, yes.
Pfft… YOU’RE the one ignoring the material reality of phenotypes and its resulting material effect IRL. Are you not the one suggesting that controlling labels will bring cis women some form of material liberation from sexism?